

Skin Cancer Statistics

Skin cancer is Australia’s most common cancer, mainly caused by UV exposure.
What is Skin Cancer?
Skin cancer is a disease in which abnormal skin cells grow uncontrollably. It usually develops due to damage from ultraviolet (UV) radiation, typically from sunlight or tanning beds, which causes mutations in the DNA of skin cells. Over time, these mutations can lead to uncontrolled cell growth and cancer.
Most aggressive Skin Cancer is melanoma (cutaneous melanoma)
A type of skin cancer in which the pigment-producing cells of the skin (melanocytes) become cancerous. It usually occurs on the parts of the body that have been overexposed to the sun, but not always. Australia and New Zealand have the world’s highest incidence of melanoma and melanoma is the third most common cancer diagnosed in Australia. The risk of being diagnosed with melanoma by age 85 is 1 in 13 for men compared to 1 in 21 for women.
What is the main cause of Skin Cancer?
Most skin cancers are caused by too much exposure to ultraviolet (UV) rays. To lower your risk of getting skin cancer, you can protect your skin from UV rays from the sun and from artificial sources like tanning beds and sunlamps.
What are signs of Skin Cancer?
Rough or scaly red patches, which might crust or bleed. Raised growths or lumps, sometimes with a lower area in the centre. Open sores (that may have oozing or crusted areas) and which don't heal or heal and then come back. Wart-like growths.
Major types of Skin Cancer
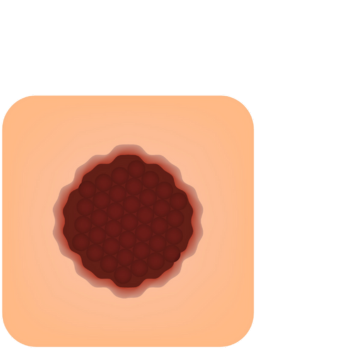
1. Basal Cell Carcinoma (BCC)
Most common type of skin cancer.
Originates in the basal cells (lower part of the epidermis).
Slow-growing and rarely spreads (metastasises).
Appearance: Pearly or waxy bump, or a flat, flesh-coloured/brown scar-like lesion.
Common on sun-exposed areas, especially the head and neck.
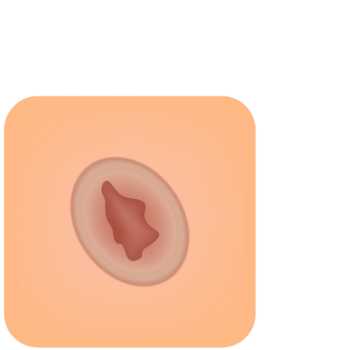
2. Squamous Cell Carcinoma (SCC)
Arises from squamous cells in the upper layers of the skin.
Second most common type.
More likely than BCC to spread, but still often treatable when found early.
Appearance: Firm red nodule, or flat lesion with a scaly, crusted surface.
Typically found on the face, ears, neck, and hands.
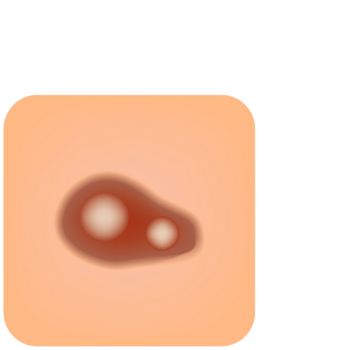
3. Melanoma
Most dangerous form of skin cancer.
Develops in melanocytes, the pigment-producing cells.
Can spread quickly to other organs if not detected early.
Appearance: Irregular, multicoloured mole or lesion that changes in size, shape, or colour.
Can occur anywhere, even in areas not exposed to the sun.
Click here to know the ABCDE warning signs of Melanoma.
Other rarer types
Merkel Cell Carcinoma – rare but aggressive, starts in hormone-producing cells.
Kaposi Sarcoma – associated with a virus, more common in immunocompromised individuals.
Cutaneous Lymphoma – cancer of lymphocytes in the skin.
Skin Cancer Statistics
Lifetime Risk
About 2 in 3 Australians will be diagnosed with some form of skin cancer before age 70 (approximately 69% lifetime risk)
Source: Cancer Council Australia
For keratinocyte cancers (non-melanoma skin cancers: BCC and SCC):
Lifetime risk is estimated at ~69% overall—73% for men, 65% for women.
Risk to age 79 is ~60% overall: 65% in men, 53% in women

Incidence & Treatment
Non‑melanoma skin cancers (keratinocyte cancers) are extremely common:
In 2022–23, there were over 1.1–1.2 million Medicare‑paid treatments for BCC and SCC combined—averaging more than 100 treatments per hour in Australia
Estimates from 2008 put the annual cases at ~434,000 (296,000 BCC and 138,000 SCC)
Melanoma (the more serious skin cancer):
In 2024, it's projected that ~18,964 Australians will be diagnosed with melanoma (third most common cancer), roughly 8% of all new cancer diagnoses
Age‑standardised incidence rate in 2020 was around 59 per 100,000(73 for males, 47 for females)
Mortality & Survival
Approximately 1,300–1,400 Australians die from melanoma each year (~ every 6 hours)
Source: Melanoma Institute Australia
Combined deaths from melanoma and keratinocyte cancers totaled an estimated ~2,105 in 2023
Five‑year relative survival for melanoma is over 90% if detected early (stage I/II)—but drops to ~26% at stage IVACD; overall 5‑year survival is around 68–94% depending on stage and timeframe
Key Takeaways
Skin cancer is the most common cancer in Australia, accounting for about 80% of all new cancer diagnoses annually.
Non‑melanoma skin cancers (BCC, SCC) dominate in sheer volume and health system burden.
Melanoma, while less frequent, causes the majority of skin cancer deaths, especially when detected late.
Men are at higher risk than women—for both incidence and mortality
Almost all skin cancers are due to UV overexposure, which makes prevention highly effective.

Why these numbers matter?
Australia's intense sun exposure, with high UV levels year-round, is a major risk driver.
Fair-skinned Australians, particularly in coastal and subtropical areas (e.g. South East Queensland), carry heightened risk—some regions see melanoma incidence nearly double the national average.
Public health efforts like Slip‑Slop‑Slap, SunSmart campaigns and skin check programs are critical—prevention and early detection dramatically improve outcomes.
Age + Location Specific Skin Cancer Statistics
Age‑Specific Breakdown
Incidence rises sharply with age—peaking in the 85–89 year age group; age‑standardised incidence rate for 2024 is estimated at 70 per 100,000overall (86 for males, 56 for females)
In 2024, a person’s lifetime melanoma risk by age 85 is about:
1 in 14 (7%) for men, and 1 in 21 (4.9%) for women
Younger Australians (<40 yrs) have seen declining incidence since the late 1990s, attributed to successful sun-safety education and demographic shifts toward lower-risk ancestries
Source: The Medical Journal of Australia
For those aged 30–39, melanoma incidence dropped from 31.4 cases per 100,000 in 2000 to 23.6 in 2024; for ages 40–49, rates rose modestly from 50.5 to 52.2 per 100,000

Variation by Postcode & Region
The Australian Cancer Atlas provides postcode-level maps showing variation in skin cancer incidence and outcomes across suburbs and postcodes
Regional and rural areas often show higher incidence and lower survival rates compared to metropolitan areas, reflecting disparities in access and sun exposure
Historically, Queensland had Australia’s highest melanoma incidence (about 64.3 per 100,000, compared to ≈48.7 nationally) in earlier data, while the Northern Territory had the lowest (~30.5)
Melanoma Stages
Cancer staging is the process of determining the amount of spread or progression of a cancer from its original site. It is one of the factors used to determine how best to treat the disease. In melanoma, there are five stages: *
Stage 0
The cancer is confined to the epidermis and has not spread. This is also known as melanoma in situ.
Stage 1
The tumour is no more than 2mm thick and might or might not be ulcerated. It has not spread.
Stage 2
The tumour is more than 1mm thick and may be thicker than 4mm. It might or might not be ulcerated. It has not spread.
Stage 3
The cancer has spread into the lymph nodes that drain the region of skin concerned.
Stage 4
There is disease outside the regional area. The melanoma has spread to distant lymph nodes or to organs such as the lungs, liver, or brain.
What you can do
Check your skin regularly – Check your skin regularly and book a skin check with a dermatologist at least once a year, or sooner if you notice any new or changing spots. Find a clinic.
Stay Sun Safe – Australia has among the highest rates of skin cancer in the world, often referred to informally as the “skin cancer capital of the world.” Click here for sun safety tips.
Avoid intentional tanning – Skip tanning beds and be wary of social media trends that glamourise sun damage. Read about the recent TikTok Tanning Challenge.
Stay informed – When detected early, melanoma is almost always curable. Even in later stages, advancements in treatment have significantly improved survival rates.
Sun Safety Tips
Australia has among the highest rates of skin cancer in the world, often referred to informally as the “skin cancer capital of the world.” Below are some tips on how you can stay sun safe.
Protect your skin from the sun
Summer // 10am - 3pm
Winter // 11am - 2pm
Wear protective clothing
(Preferably long sleeves and a collar)
Wear a broad brimmed hat
Use and reapply sunscreen every 2 hours
(spf 50+)
Wear sunglasses

Seek shade